




Disclaimer and Disclosures: This is an informational resources page/guide and should NOT be used in lieu of training. We hope in this difficult time it will act as a general guide, but specifics of implementation depend on several and complex factors that cannot be fully considered in this format. Click here to see Dr. Malandraki's disclosures.
To cite this page:
Malandraki, G.A. (2020, April 24). Telehealth Recommendations for Dysphagia Management during COVID-19. Purdue I-EaT Lab. https://www.purdue.edu/i-eatlab/telehealth-resources-for-dysphagia-management-during-covid-19/
This introductory section dives into the basics of telehealth and provides important definitions. It includes the following 5 sections:
- What does telemedicine, telehealth, and telepractice mean? It may surprise you, but these definitions may vary from State to State!
- What are some misconceptions about telehealth SLP services?
- What are the aims and responsibilities when using this service delivery model?
- What do the terms “synchronous”, “asynchronous” etc. mean, in general and particularly for dysphagia care?
- Test your knowledge on Part A of this guide with this self-quiz!
1. What does telemedicine, telehealth, and telepractice mean? It may surprise you, but these definitions may vary from State to State!
Telemedicine is defined as “the use of electronic information and telecommunications technologies to provide and support health care when distance separates the participants” (Telemedicine, 1996), therefore it includes the provision of remote clinical services. Telehealth is a broader term that refers to “the use of electronic information and telecommunications technologies to support long-distance clinical health care, and also patient and professional health-related education, public health and health administration” (Health Resources and Systems Administration (HRSA), 2019). ASHA prefers the term telepractice because it encompasses our practices that are provided both inside and outside health care settings (e.g., schools), and provides the following definition for telepractice “..the application of telecommunications technology to the delivery of speech language pathology and audiology professional services at a distance by linking clinician to client/patient or clinician to clinician for assessment, intervention, and/or consultation” (ASHA Telepractice Portal).
The phrase “telecommunication technologies” appears in all these definitions and could mean a wide variety of technologies, i.e., phones, texts, emails, live video-conferencing, and more. However, these terms may be defined differently in different states and laws statutes. For example in Indiana, telemedicine is defined as “delivery of health care services using electronic communications and information technology, including: (1) secure videoconferencing; (2) interactive audio-using store and forward technology; or (3) remote patient monitoring technology” (Indiana General Assembly 2020 Session). This excludes the use of phone, texts, or emails, for example. Although this seems logical, we have to consider scenarios of patients without Internet or computer access, when phone communication may be the only available remote technology.
Therefore, it is imperative that clinicians are aware of the specific definitions provided by their State legislation. ASHA has recently provided pdf resources that are frequently updated with collective information about each state’s regulations (ASHA Coronavirus Updates). In addition, the Center for Connected Health Policy updates their website regularly to provide information on the continuously evolving changes occurring within the COVID-19 environment and also includes state-by-state interactive maps regarding these policies (CCHPCA). State Associations have to play a critical role in helping clinicians in each state navigate these uncharted waters. A silver lining in this difficult situation is that many State Associations are becoming very active in this area and new state laws and statutes are emerging on a regular basis. Being a member of State Associations and being actively involved is probably now more important than ever and will be very beneficial.
2. What are some misconceptions about telehealth SLP services?
In the last month, the amount of discussions about telehealth services for speech language pathologists in social media has skyrocketed. This may eventually be another highly positive silver lining of this dire situation for our profession and our patients. However, this explosion of communications on the matter has also resulted in several misconceptions, fears for the unknown, and erroneous strong opinions. Telehealth/telepractice is a service delivery model; just like in-person management is another service delivery model. It IS NOT a clinical service per se. It is another way to offer the services we have already been trained to offer. However, just as in-person service delivery requires guidelines to be followed, special tools, training, and practice, the use of telehealth should also follow basic guidelines, training, use of specific tools, and require some practice. In many situations it also requires the use of trained facilitators, a.k.a. e-helpers [see section on facilitators and training in Practical Guidelines]. These facilitators/e-helpers are not there to replace us. They should be trained/instructed (by us) and their role is to facilitate patients in the use of technology, environmental requirements (e.g., use of appropriate lighting and noise) (Alvares, 2013; Tucker, 2012), and possibly in completing the tasks we need them to perform to make our diagnostic and therapeutic conclusions (e.g., help with testing during a cranial nerve assessment) (e.g., Malandraki, Roth, & Sheppard, 2014; Sharma, Ward, Burns, Theodoros, & Russell, 2012). No nurse, caregiver, radiology technician, or teacher is trained to complete and interpret a comprehensive clinical swallowing evaluation, a VFSS assessment, or complete a treatment session. The SLPs (in most states in the US) are the ones with training to complete, interpret, and guide dysphagia evaluations and care, irrespective of the service delivery modality used.
Another related misconception is that teleheatlh services should be billed at a lower rate than in-person services. That is simply NOT valid. The services we provide are based on our professional training, years of education and practice, and our expertise in our respective areas. All these qualifications do not go away when we use telehealth. The services one provides via telehealth should be equal or not inferior to services offered in-person. If one does not believe that the services they can offer via telehealth are equivalent to in-person services, they should not provide these services; not just charge less for them.
3. What are the aims and responsibilities when using this service delivery model?
According to the Center for Connected Health Policy and the Telehealth Resource Centers “there should be NO regulatory distinction between a service delivered via telehealth and a service delivered in person (Telehealth Resource Centers, 2018) (CCHPCA Definition of Telehealth). This means that when treating someone via telehealth we have the exact same responsibilities and regulatory oversight, as we do when we are treating them in-person.
 ASHA also highlights this point in the statement “Use of telepractice must be equivalent to the quality of services provided in person and consistent with adherence to the Code of Ethics (ASHA, 2016a), Scope of Practice in Audiology (ASHA, 2018), Scope of Practice in Speech-Language Pathology (ASHA, 2016b), state and federal laws (e.g., licensure, Health Insurance Portability and Accountability Act) and ASHA policy” on their website. In today’s unprecedented situation some adjustments will have to be made, just as we need to make adjustments to continue offering in-person services. However, these adjustments should be made with extra care for procedural, legal, ethical, and practical standards established by our nationally recognized professional organizations (Richmond et al., 2017).
ASHA also highlights this point in the statement “Use of telepractice must be equivalent to the quality of services provided in person and consistent with adherence to the Code of Ethics (ASHA, 2016a), Scope of Practice in Audiology (ASHA, 2018), Scope of Practice in Speech-Language Pathology (ASHA, 2016b), state and federal laws (e.g., licensure, Health Insurance Portability and Accountability Act) and ASHA policy” on their website. In today’s unprecedented situation some adjustments will have to be made, just as we need to make adjustments to continue offering in-person services. However, these adjustments should be made with extra care for procedural, legal, ethical, and practical standards established by our nationally recognized professional organizations (Richmond et al., 2017).
4. What do the terms “synchronous”, “asynchronous” etc. mean, in general and particularly for dysphagia care?
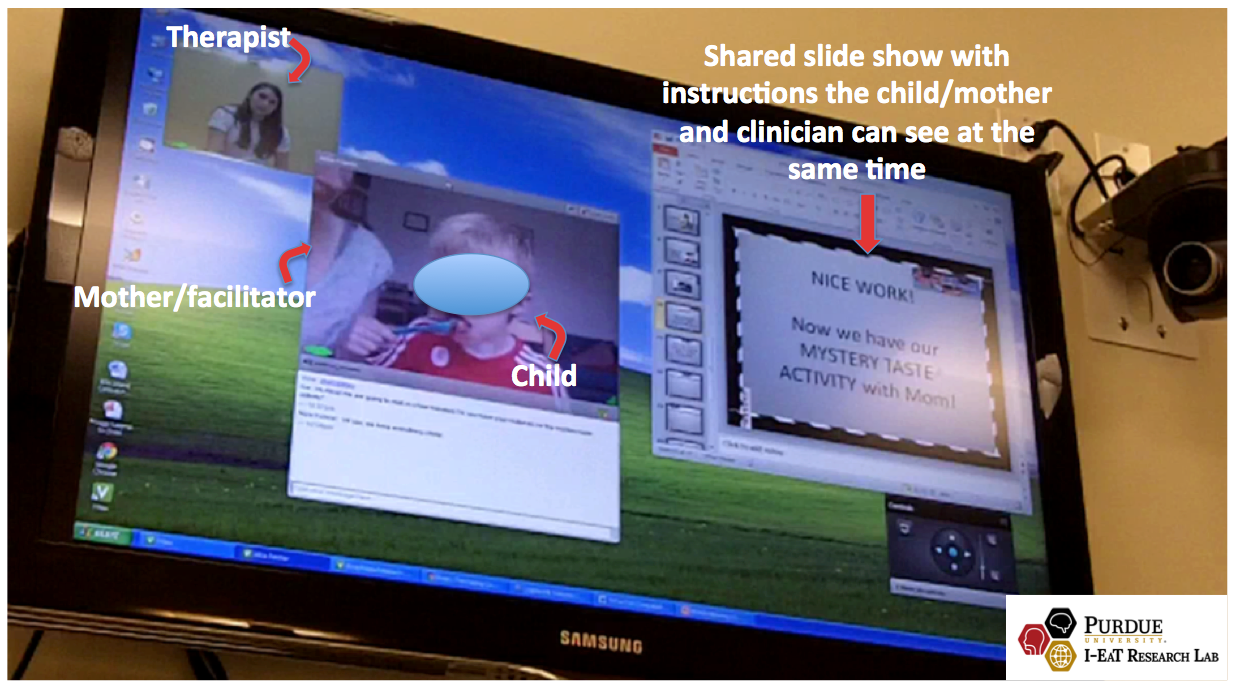
These are several ways telehealth can be provided. Most individuals are familiar with what is known as synchronous methods. These include live video conferencing and immediate interaction between clinician and patient or clinician and clinician (for consultation purposes) (HRSA, 2019; Wilson & Maeder, 2015). In dysphagia telehealth literature synchronous methods have been used both for tele-evaluations (tele-clinical and tele-VFSS assessments) and tele-treatment provision with positive results (e.g., Burns, Ward, Hill, Phillips, & Porter, 2016; Burns et al., 2017; Malandraki, McCullough, He, McWeeny, & Perlman, 2011; Malandraki et al., 2014; Raatz, Ward, Marshall, & Burns, 2019; Ward et al., 2009; Ward et al., 2012; Ward, Burns, Theodoros, & Russell, 2013; and more).
Asynchronous methods include the acquisition of video recordings, audio recordings or images that are stored and transmitted (i.e., stored and forwarded) for interpretation by a medical professional. Therefore, in asynchronous systems 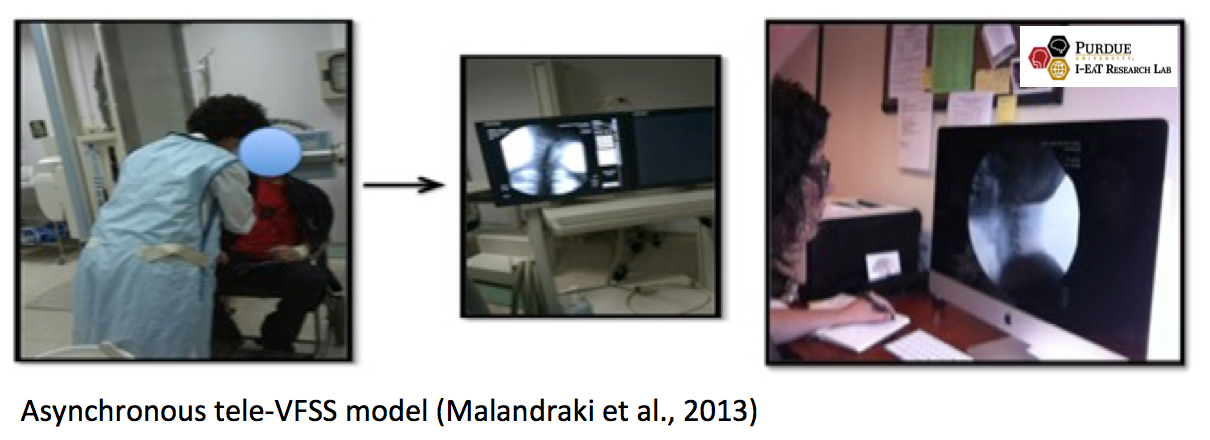 the components of interactionare de-coupled and occur at different times (Wilson & Maeder, 2015). Asynchronous methods can also be valuable in dysphagia care (Kantarcigil & Malandraki, 2016; Malandraki et al., 2013),with a study showing that asynchronous consultations offered by an expert dysphagia specialist on stored and forwarded VFSS evaluations resulting in up to 50% improvement in the quality of care provided (Malandraki et al., 2013). Hybrid telehealth models include any number of combinations of synchronous, asynchronous, and/or in-person services.
the components of interactionare de-coupled and occur at different times (Wilson & Maeder, 2015). Asynchronous methods can also be valuable in dysphagia care (Kantarcigil & Malandraki, 2016; Malandraki et al., 2013),with a study showing that asynchronous consultations offered by an expert dysphagia specialist on stored and forwarded VFSS evaluations resulting in up to 50% improvement in the quality of care provided (Malandraki et al., 2013). Hybrid telehealth models include any number of combinations of synchronous, asynchronous, and/or in-person services.
5. Test your knowledge through this self quiz!
- What is the difference between telehealth and telepractice?
- True or False: Telemedicine and telehealth are defined differently in different states. If false, correct the statement and explain why.
- Fill in the blank: Telehealth/telepractice is a ____________________, NOT a clinical service.
- True or False: Telehealth services should be billed at a lower rate than in-person services. If false, correct the statement and explain why. If false, correct the statement and explain why.
- What is the difference between synchronous and asynchronous methods in telepractice for dysphagia care?
Content created by Dr. Georgia A. Malandraki, Ph.D., CCC-SLP, BCS-S / Web support/development: Samantha Mitchell






